Strategy is guaranteed to fail when it’s built on bad data
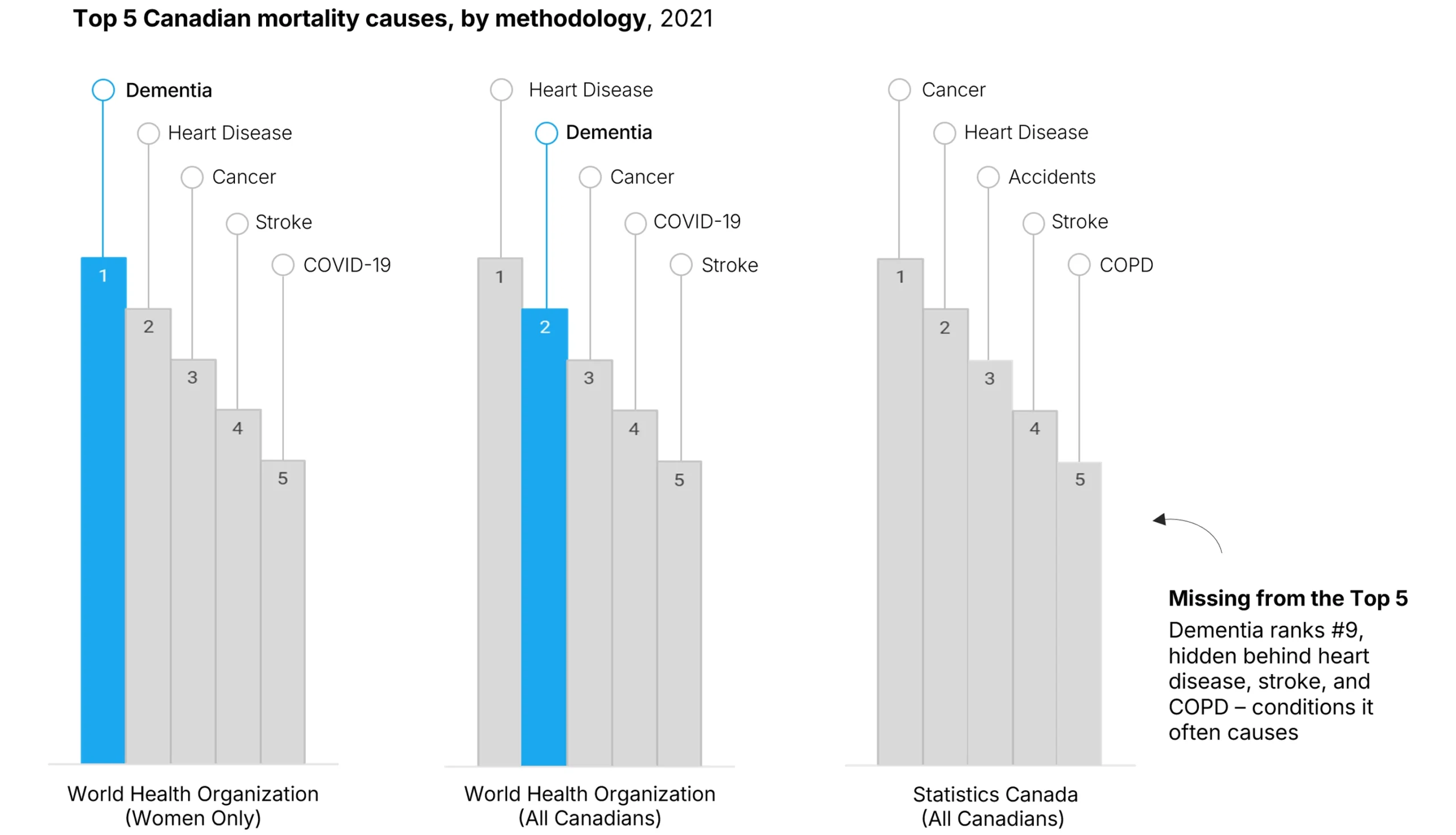
Picture this scenario: You're a Canadian healthcare policymaker faced with the daunting task of making tradeoffs among many worthy programs. You look to Statistics Canada mortality data to help you prioritize where to invest. Their data ranks cancer and heart disease as Canada's top two killers, so you prioritize spending in those areas. The same data ranks dementia a distant ninth, so you defer any meaningful spending on dementia policy.
But how would your spending priorities change if dementia was Canada's leading cause of death for women and second for the general population? Because it already is, according to The World Health Organization. Furthermore, dementia's economic burden reached $40.1 billion in 2020 and is projected to surge to $153 billion annually by 2038, a 275% increase. The adage that you can't manage what you don't measure has come true for Canada's dementia policy, creating a dangerous blind spot in healthcare planning.
Sources: Mortality data sourced from WHO Global Health Estimates and Statistics Canada "Deaths and age-specific mortality rates, by selected grouped causes" (Table 13-10-0392-01). Economic projections from Canadian Health Policy Institute showing $40.1 billion annual burden rising to $153 billion by 2038. Specialist workforce analysis based on Black et al., "A Model Predicting Healthcare Capacity Gaps For Alzheimer's Disease-Modifying Treatment in Canada," Canadian Journal of Neurological Sciences (2024), identifying need for 14-fold increase in specialists. National Dementia Strategy funding data from Government of Canada 2024 annual report.
How can two authoritative sources produce such different rankings? This striking discrepancy emerges from fundamentally different approaches to death certification. The WHO recognizes dementia as the underlying cause of death when it initiates the cascade of health complications that ultimately lead to mortality. In contrast, Statistics Canada codes the immediate complications (heart disease, stroke, or COPD) that dementia patients experience in their final stages. This systematic undercounting creates a false impression that dementia represents a manageable ninth-place health challenge rather than the population health crisis it actually represents.
The policy implications of this data misalignment are profound. When fundamental disease burden statistics are systematically understated, it creates structural impediments to appropriate resource allocation and specialist training. Canada's investment priorities reflect this misalignment: the National Dementia Strategy received only $50 million over five years (a 67% shortfall from stakeholder recommendations) while single infrastructure projects like Ontario's $400 million parking garage receive immediate political priority. Research by Black et al. shows that meeting projected demand would require a 14-fold increase in Alzheimer's disease specialists, a gap that would take over 100 years to close under current training pipelines.
Canada needs to fix its dementia data problem. The Netherlands did this in 2013 by switching to WHO coding standards, which immediately showed 20% more dementia deaths. It was politically uncomfortable but led to better policies. Canadian healthcare leaders must stop using incompatible data sources and adopt shared measurement standards. Organizations that help align government, hospitals, and insurers around accurate dementia statistics will unlock better resource decisions and save lives.
About the author
Mark McCarvill is the Founder and Lead Facilitator at Mind Meeting Group, a strategy consulting firm based outside Vancouver, Canada. Mind Meeting Group helps business, government, and non-profit leaders align departments and mobilize teams through collaborative workshops that deliver execution-ready strategies.